 |
The sonographic diagnosis of acute appendicitis is based on identification of a tubular, noncompressible, aperistaltic bowel loop, which demonstrates a connection with the cecum and a distal blind end, with a diameter greater than 6 mm |
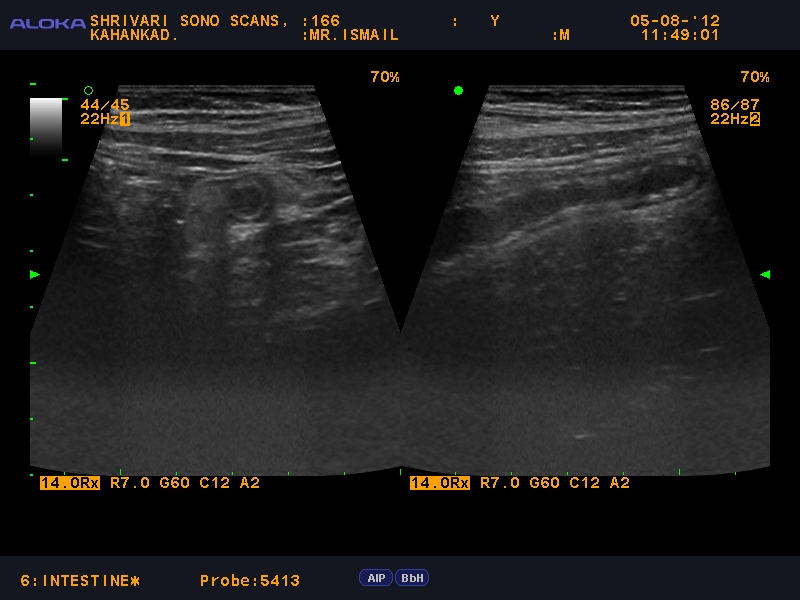 |
ultrasound of the right lower quadrant with the appendix showing the
"target" sign seen in acute appendicitis..
Graded
compression ultrasonography is one of the two imaging modalities commonly used in the
assessment of
clinically suspected appendicitis..
This
self-localization technique has a sensitivity of 85%, specificity of 60%, and
accuracy of 75% in diagnosing appendicitis. The overall accuracy of this
technique in diagnosing appendicitis as well as other significant disease
processes which may clinically mimic appendicitis is 86%. However, the
self-localization technique is of limited value with retrocecal or perforated
appendicitis due to the patient's inability to accurately localize the pain
(21).
Based on
the data of several recent studies, CT performed for clinical suspicion of appendicitis with atypical symptoms has a sensitivity of 87 - 96%, specificity of 89 - 97%, positive
predictive value of 95%, negative predictive value of 95%, and accuracy of 94% (27,29).
|
 |
| Perforated appendix with local peritonitis |
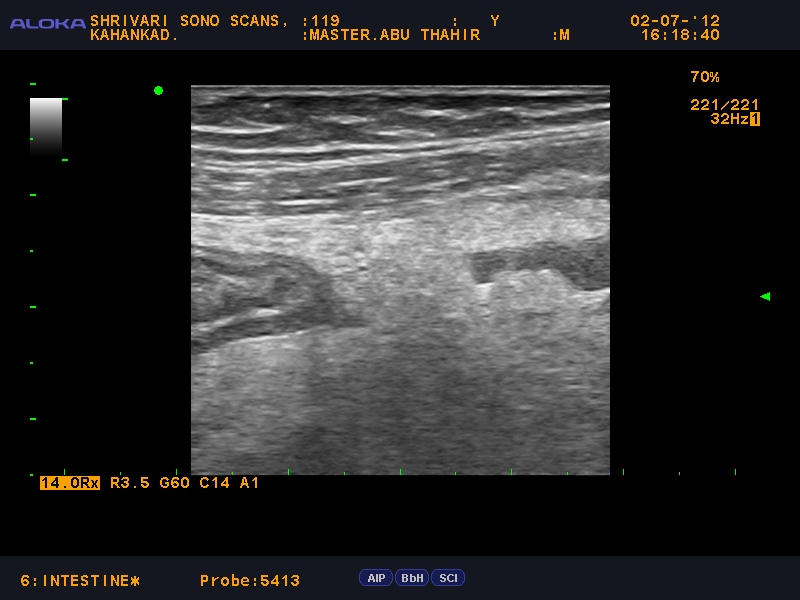 |
| inflammed appendix with echogenic edematous omentum around |
 |
| acute appendicitis |
 |
| Retrocaecal appendix |
 |
| retrocaecal appendix showing target sign. |
 |
| Inflammed tip of the appendix. |





































