|
Retinopathy
of prematurity is seen in low birth weight premature infants due to abnormal
postnatal growth of retinal vasculature.
ULTRASONOGRAPHY
HELPS TO DIFFERENTIATE IT FROM OTHER CAUSES OF LEUKOCORIA.
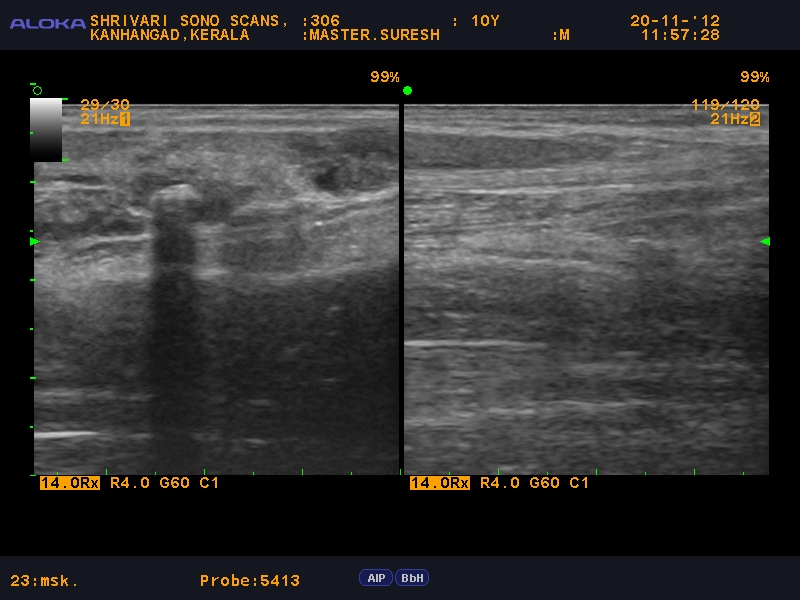
Ultrasonography reveals bilateral small sized eyes with funnel shaped
high reflective membrane attached to the optic disc suggestive of total retinal
detachment..
|
 |
Axial B
scan image shows funnel shaped highly reflective membrane inserting into the
optic disc.
Accumulation of echoes in the anterior part suggesting the presence
of preretinal fibrous tissue.
|
 |
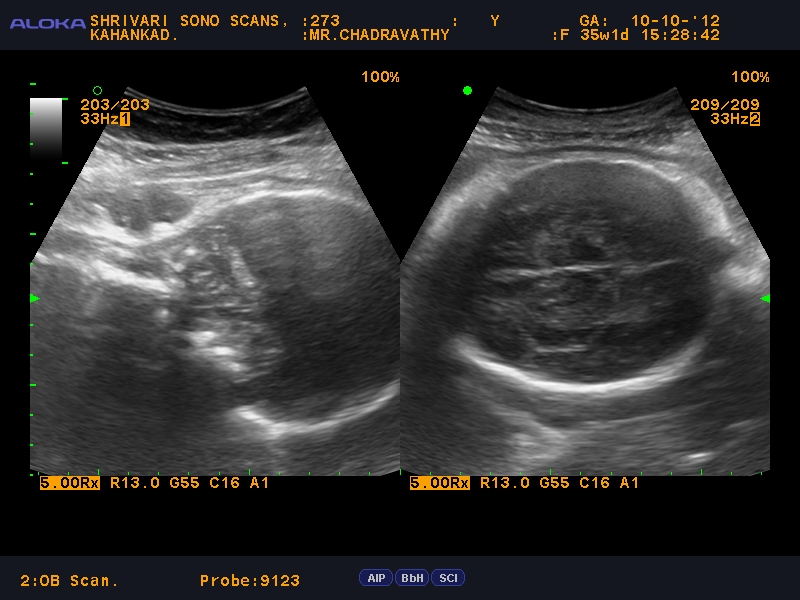
Axial B scan reveals the exact configaration of
the funnel
|
 |
| The B scan image shows packed retrolental echoes with retinal detachment |